Shahd, a 12-year-old girl with a hearing disability, stands in front of a window facing her father, in the house her family live in, Azaz, Aleppo, Syria. Credit: Human Rights Watch.
Opinion by Emina Cerimovic (new york)
Inter Press Service
NEW YORK, Feb 28 (IPS) – Emina Cerimovic is a senior disability rights researcher at Human Rights Swatch.A few days ago, I saw a photo shared to Twitter of Sham, a young Syrian girl rescued from under the rubble in northwest Syria, sitting upright in her hospital bed, According to the Syrian Civil Defense, a volunteer humanitarian group also known as the White Helmets, Sham will lose both her legs because of injuries from the quake.
Looking at her photo, I couldn’t help but think of the additional human rights abuses Sham will experience on the basis of her disability. She will join the ranks of all the children with disabilities who are surviving the 12-year-conflict in Syria without equal access to humanitarian aid.
And so will others who experienced traumatic physical and psychological injuries in the wake of the earthquakes: a girl who had spent 30 hours under the rubble in the heavily affected town of Jindires in northwest Syria and who had lost both her legs; a 3-year-old boy in Jinderis who was trapped for 42 hours and whose left leg was amputated; a young Syrian man living in Gaziantep, Turkey, whose right hand was amputated.
As issues of humanitarian aid access to various affected parts of Syria dominatethe news, relief efforts should not overlook the short and long-term needs of people with disabilities and the thousands of earthquake survivors who have sustained physical and psychological injuries that could lead to permanent disabilities.
As two more powerful earthquakes struck the region on February 20, panic and fear spread among earthquake survivors in both Syria and Turkey, bringing into sharp focus the psychological trauma caused by the natural hazard and, for Syrians, by over 12 years of war.
In Syria, approximately 28 percent of the current population – nearly double the global average – are estimated to have a disability, and their rights and needs are largely unmet. As I found in my September report on the greater risk of harm and lack of access to basic rights for children with disabilities caught up in the Syrian war, the design and delivery of humanitarian programs in Syria are not taking into account the particular needs of children with disabilities. In some cases, such programs explicitly exclude them.
As an example, some educational activities and child-friendly spaces excluded children with intellectual and developmental disabilities. Children with disabilities are growing up without safety, basic necessities, education, assistive devices, or psychosocial support, in ways that put their lives and rights at risk.
They experience stigma, psychological harm, and higher levels of poverty. The situation is no better for adults with disabilities who also face systematic challenges in accessing humanitarian services on an equal basis with others.
This crisis should serve as a wake-up call for UN agencies, donor states, humanitarian organizations, and charities to properly respond to all children’s rights by ensuring the rights and needs of children with disabilities are also met.
They should develop and implement their response and recovery action plans with people with disabilities at their core. The attention and investment in children – like Sham – and adults with disabilities will enhance human rights for everyone.
These are the first cases of avian influenza, known as H5N1, reported in Cambodia since a widespread outbreak in 2014, the World Health Organization (WHO) said. The infection, which largely affects animals, has a 50 per cent mortality rate in humans.
“The global H5N1 situation is worrying given the wide spread of the virus in birds around the world,” said Sylvie Briand, Director for Epidemic and Pandemic Preparedness and Prevention at the UN health agency. “We are in close communication with the Cambodian authorities to understand more about the outbreak.”
Further cases expected
Since the virus continues to be detected in poultry populations, further human cases can be expected, WHO said. Almost all H5N1 infection cases in people have been associated with close contact with infected live or dead birds or contaminated environments.
“WHO takes the risk from this virus seriously and urged heightened vigilance in all countries,” she said.
From 2003 to 25 February 2023, a total of 873 human cases of H5N1 and 458 deaths have been reported globally in 21 countries.
However, based on the current information, WHO advises against applying any travel or trade restrictions. To date, evidence shows that the virus does not infect humans easily and person-to-person transmission appears to be unusual.
Investigations launched
In Cambodia, a joint animal-human health investigation is already underway in Prey Veng province, where the case was reported. It aims at identifying the source and mode of transmission.
Meanwhile, a high-level government response is working to contain any further spread of the virus, and an outbreak investigation is aimed at determining the exposure of the two reported cases to the virus, WHO said.
Cambodian health authorities had notified WHO on Thursday of the first case and death. A young girl had contracted the avian flu and had died on Wednesday. By Friday, they had reported the second case, noting that one of the girl’s family members had tested positive with the virus but was asymptomatic.
FAO/Hoang Dinh Nam
In response to past outbreaks, veterinary efforts to contrast avian influenza strains were bolstered across Asia.
Global response system
Through its Global Influenza Surveillance and Response System, the UN health agency monitors the evolution of the virus and conducts risk assessments. For pandemic preparedness purposes, WHO can also recommend the development of additional new candidate vaccine viruses.
The agency underlined the importance of global surveillance to detect and monitor virological, epidemiological, and clinical changes associated with emerging or circulating viruses that may affect human or animal health.
Currently, there is no vaccine widely available to protect against avian influenza in humans. WHO recommends that all people involved in work with poultry or birds should have a seasonal influenza vaccination to reduce potential risks.
In 2015, FAO again raised alarms about a dangerous outbreak of the highly virulent H5N1 strain, which had spread to five West African countries within six months. The agency had appealed for $20 million in emergency funds “to stop it in its tracks” before it affected humans.
At the time, FAO had said the H5N1 strain has caused the death of tens of millions of poultry and losses of tens of billions of dollars.
Since then, the agency has worked to improve veterinary systems and the capabilities of local laboratories. By 2018, FAO had trained 4,700 veterinarians, who worked to protect farm animals against deadly viruses in 25 countries across Africa, Asia, and the Middle East.
In Cambodia, a 2003 H5N1 outbreak had, for the first time, affected wild birds. Since then, and until 2014, human cases due to poultry-to-human transmission have been sporadically reported in the country.
As of 25 February, Cambodia has reported a total of 58 cases of human infection with the H5N1 virus have been reported since 2003, including 38 deaths.
The two processes are complementary, guided by the imperative of making the world safer from communicable diseases and ensuring equitable responses to public health threats, said Ashley Bloomfield, former Director-General of Health of New Zealand, who co-chairs the working group on updating the 2005 WHO International Health Regulations, which concluded its latest round of discussions on Friday.
“The efforts to update the International Health Regulations and draft apandemic accord share a number of common themes, including the importance of equity in access to health, collaboration and capacity building,” he said. “It is important that there is consistency and alignment across the two processes.”
Facing COVID-19 challenges
A total of 307 amendments to the WHO International Health Regulations came in response to challenges posed by the COVID-19 pandemic. As of Tuesday, WHO reported a total of 757,264,511 confirmed cases, including 6,850,594 deaths, since the start of the pandemic in 2020.
“COVID-19 showed us that having a good, strong set of international health regulations is essential, and showed where the current regulations need to be improved,” Dr. Bloomfield said.
During the week-long working group session, he said governments had focused on making their countries, and the international community, better prepared for future emergencies. They also stressed the importance of enhancing capacity building, especially in low-income countries; access to benefits arising from sharing pathogens; equitable access to medical countermeasures; and enhanced cooperation and information sharing.
Making the world safer
“The ongoing pandemic has underscored the importance of countries working together collaboratively, and supporting WHO in its vital work, to make the world safer,” he said. “The tone of the discussions and progress made during this week’s meeting clearly show that countries understand the responsibility they have to ensure this process is successful.”
Abdullah M. Assiri, Saudi Arabia’s Deputy Minister of Health and working group co-chair, said the 194-nation WHO membership is “in the driving seat” of the process of strengthening the current regulations.
“During the pandemic, the world faced the urgent need for functioning international instruments, and placed increasing importance in international organizations, such as WHO,” he said. “Updated regulations will enable the world to better detect outbreaks early and prevent them from developing into public health emergencies of international concern. This is about strengthening our collective ability to do that and to better protect everybody.”
The 2005 regulations had set out agreed approaches and obligations for countries to prepare for, and respond to, disease outbreaks and other acute public health risks. The working group is set to meet again in April to continue discussions.
The WHO working group met to consider 307 amendments proposed by governments to update current regulations.
New ‘pandemic accord’
On Monday, governments will begin negotiating the drafting of a WHO instrument on pandemic prevention, preparedness, and response. Referred to as a pandemic accord, the “zero draft” of the agreement will be the focus of discussions during the week-long session.
Calls for action to draft the accord came following the World Health Assembly’s special session in December 2021, in recognition of the failure of the international community in showing solidarity and equity in response to the coronavirus pandemic.
Global health strides
The International Sanitary Regulations, issued in 1951, preceded the landmark 2005 WHO regulations. Both follow more than a century of global health strides, dating back to the first International Sanitary Conference, held in Paris in 1851, which drafted quarantine regulations to stem the spread of cholera, yellow fever, and other deadly pandemics at the time.
At the UN General Assembly’s first-of-its-kind science session, held in early February, epidemiologists and researchers had called for a global pandemic warning system. Suggestions included forging a new global digital collaboration comprising a network of researchers connected through an open-source data science platform capable of quantifying, modeling, and ultimately solving any climate and health problem at any scale.
Three countries, this week alone, have reported outbreaks, WHOcholera team leader Philippe Barboza told reporters at a press conference on Friday.
For the first time, WHO is asking donors for help to fight the outbreaks, he said.
Right now, 22 countries across the world are fighting outbreaks of the acute diarrhoeal infection caused by eating or drinking contaminated food or water. Cholera cases climbed in 2022, following years of falling numbers of cases, and the trend is expected to continue into this year, he said.
He said cases have been reported in five of the six regions where WHO operates. The latest WHO global overview published in early February showed the situation has further deteriorated since 2022.
Poverty, disasters, conflict and climate change consequences continue to be driving factors alongside a lack of access to safe water and sanitation, Dr. Barboza said.
Limited vaccine supplies
“An unprecedented situation requires an unprecedented response,” he said, drawing attention to the limited availability of vaccines, medicines, and testing kits.
Only 37 million doses are available in 2023, he said. More doses are expected to be available by next year.
As a result of the current global surge, WHO is, for the first time ever, appealing to donors to support a $25 million fund to help to address cholera outbreaks and save lives, he said.
Prevention is key, he said, noting that nearly half of the world lacks access to safely managed sanitation.
“Access to safe drinking water and sanitation are internationally recognized human rights,” he said. “Making these rights a reality will also end cholera.”
Outbreak in Africa
An exponential rise in the number of cholera cases in Africa includes an outbreak in Mozambique, which is also grappling with severe storms brought on by cyclone Freddy. The first case of cholera in the current outbreak was reported to the Ministry of Health and WHO from Lago district in Niassa province in September.
As of 19 February, Mozambique reported a cumulative total of 5,237 suspected cases and 37 deaths. All six cholera-affected provinces are flood-prone areas, and WHO anticipates that more will be affected as the rainy season continues.
Considering the frequency of cross-border movement and the history of cross-border spread of cholera during this outbreak, WHO considers the risk of further disease spread as very high at national and regional levels.
An estimated 26,000 cases and 660 deaths have been reported as of 29 January 2023 in 10 African countries facing outbreaks since the beginning of the year, WHO said. In 2022, nearly 80,000 cases and 1,863 deaths were recorded from 15 affected countries.
Multiple countries affected
Neighbouring Malawi is facing the deadliest cholera outbreakin two decades, and cases are being reported in other countries, including Ethiopia, Kenya and Somalia, WHO reported.
The UN health agency said challenges include climate change, which has led to drought or flooding in parts of Africa, resulting in increased population displacement and reduced access to clean water.
Worldwide, people in Haiti, India, Pakistan, the Philippines and Syria, among others, are also affected by outbreaks.
Global threat
Cholera remains a global threat to public health, WHO said. In 2017, affected countries, donors, and partners of the Global Task Force on Cholera Control launched a renewed global cholera control strategy, Ending Cholera: A Global Roadmap to 2030. It aims at reducing cholera deaths by 90 per cent over the next decade.
While the number of cases had been declining, WHO remains concerned about the current surge. Researchers estimate that every year, there are between 1.3 and 4 million cases and 21,000 to 143,000 deaths worldwide due to the infection.
ISLAMABAD, Pakistan, Feb 24 (IPS) – While its origins may be rooted in the discrimination faced by people living with HIV, Zero Discrimination Day has evolved to celebrate commitments to the fundamental human right of being treated equally in law and in practice.
Within the context of global health, the day is an opportunity to examine discrimination from the perspective of health and care workers, who face barriers based on their race, gender, and other socio-economic and cultural factors.
In the context of a global health workforce under siege from the threat of the great resignation in health, it is especially important to examine the impact of discrimination on health systems at global, national and local levels.
In recent times, recognition of the gender pay gap in health of 24% and its impact on national and regional economy has spurred greater research into the unequal treatment of women, taking into account their specific contexts and locations. Despite efforts to address these issues, progress has been uneven.
Mounting evidence around gender inequities in the health workforce, specifically at the leadership level underscores the problem of gender bias in health decision-making. Women who make up 70% of the overall health workforce and 90% of frontline staff continue to be marginalised in leadership, occupying just one-quarter of the decision-making roles in health.
Furthermore, occupational segregation and the clustering of women into low-earning professions and settings further limit their career advancement. Their experiences in the health workforce are further compounded by various forms of discrimination, such as harassment, violence, assault and discrimination at several levels.
Gender is not the only factor at play. As health workers migrate from rural and remote areas to well-resourced urban centres, or from developing to developed countries, new forms of barriers and biases emerge in a global context where high-income nations wield most of the socio-economic power.
These include the need to undergo resource-intensive accreditation and licensing exams, encountering anti-immigrant hostility and changing patient-provider dynamics, limited options from smaller job pools, and being affected by global events and geopolitical shifts.
This “brain drain” of health workers also has negative implications for the understaffed health systems that they leave behind.
In addition to gender and migrant status, healthcare workers may also face discrimination based on their race, ethnicity, language and dialect, marital status and sexual orientation, amidst other factors. These experiences affect the health workforce in different ways, resulting in inefficiencies, demotivation and burnout at the local, national and regional levels.
Healthcare systems that fail to acknowledge and address latent discriminatory actions may unintentionally perpetuate these inequalities, further exacerbating the biased experiences of healthcare workers, despite the need for a diverse health workforce to better serve their diverse populations.
While we talk about zero discrimination, dignity, decent work, fair pay, and the importance of endorsing diversity and practising inclusion at the macro level of health systems, are we also ‘seeing’ and ‘acknowledging’ where this discrimination exists and understanding the negative consequences on health workers and population’s health? Are we collecting and analysing the data that give us the full picture?
More importantly, discrimination in healthcare settings not only violates the fundamental human right to be treated with respect and equality, but also severely limits the chances of achieving the SDGs by 2030. The 2017 UN statement succinctly framed this understanding in their call to end discrimination in healthcare settings.
Equal opportunities and experiences for health and care workers must be ensured at every stage of their career, including recruitment, promotion, growth and advancement, particularly in the post-COVID era of globalisation.
Gender and race are the primary drivers of inequality, around which most of the structural discrimination in health revolves. Therefore, policies and practices must be devised to study and address this discrimination and their underlying drivers, to fully exploit the available talent and potential of the health workforce and to ensure equitable opportunities for growth and leadership and strategically achieve UHC.
Now more than ever, it is urgent that leaders in global health take bold action by committing to a new social contract that prioritises the rights of health and care workers. This step will not only ensure a more equitable and just health workforce, but also provide better health outcomes for communities worldwide.
Roomi Aziz is Technical Lead of the Pakistan Chapter, Women in Global Health
According to a new report from the World Health Organization (WHO), maternal deaths have either increased or stagnated nearly everywhere, from 223 maternal deaths per 100,000 live births in 2020, down from 227 in 2015 and 339 in 2000.
Unless progress is made on global targets for reducing maternal deaths – most of which are preventable – the lives of over one million more women by 2030 could be at risk, the WHO warned.
“Pregnancy … is tragically still a shockingly dangerous experience for millions around the world who lack access to high quality, respectful health care,” said Tedros Adhanom Ghebreyesus, the WHO Director-General.
Tedros highlighted stark disparities in healthcare access in many regions and the urgent need “to ensure every woman and girl has access to critical health services before, during and after childbirth, and that they can fully exercise their reproductive rights”.
Furthermore, as the world slowly emerges from the COVID-19 pandemic which has highlighted that coronavirus infections can increase risks during pregnancy, the report’s authors stressed that more research will be needed to show the true impact of the global health emergency on maternal deaths.
Baby steps
The WHO-produced report, Trends In Maternal Mortality, tracked maternal deaths nationally, regionally and globally from 2000 to 2020.
It calculated 287,000 maternal deaths worldwide in 2020, which represented “only a slight decrease” from 309,000, in 2016.
This was the case despite countries’ pledges in 2015 to implement the Sustainable Development Goals (SDGs), whose target is less than 70 maternal deaths per 100,000 live births by 2030.
Although the report indicated “some significant progress” in reducing maternal deaths between 2000 and 2015, gains largely stalled, or in some cases even reversed, after this point, its authors said.
Responding to the report’s findings, the UN Population Fund’s (UNFPA) Executive Director, Dr. Natalia Kanem expressed alarm that “so many women continue to die needlessly in pregnancy and childbirth. Over 280,000 fatalities in a single year is unconscionable.”
Dr. Kanem added: “We can and must do better by urgently investing in family planning and filling the global shortage of 900,000 midwives so that every woman can get the lifesaving care she needs. We have the tools, knowledge and resources to end preventable maternal deaths; what we need now is the political will.”
Maternal care services are close to a standstill in Haiti.
Conflict and poverty: a deadly cocktail
Among the report’s key findings: that maternal deaths remain largely concentrated in the poorest parts of the world and in countries affected by conflict.
In 2020, about 70 per cent of all maternal deaths were in sub-Saharan Africa. And in nine countries facing severe humanitarian crises, maternal mortality rates were more than double the world average (551 maternal deaths per 100,000 live births, compared to 223 globally).
The leading causes of maternal death are severe bleeding, high blood pressure, pregnancy-related infections, complications from unsafe abortion and underlying conditions that can be aggravated by pregnancy – such as HIV/AIDS and malaria.
“These are all largely preventable and treatable with access to high-quality and respectful healthcare,” the report’s authors stressed.
Additional data showed that roughly one-third of women do not receive four of the recommended eight antenatal checks or receive essential postnatal care, while some 270 million women lack access to modern family planning methods.
The report’s authors also stressed that inequality related to income, education, race or ethnicity “further increase risks for marginalized pregnant women, who have the least access to essential maternity care but are most likely to experience underlying health problems in pregnancy”.
The report was produced by WHO on behalf of the UN Maternal Mortality Estimation Inter-Agency Group comprising WHO, UNICEF, UNFPA, the World Bank Group and the Population Division of the United Nations Department of Economic and Social Affairs (DESA).
A girl reads a story book with lessons on life skills at an ELA club in Uganda. Credit: Uganda/BRAC
by Naureen Hossain (united nations)
Inter Press Service
UNITED NATIONS, Feb 22 (IPS) – BRAC’s Empowerment and Livelihood Program (ELA) has benefitted tens of thousands of girls, and its recently released report shows an organization willing to adapt to the circumstances to continue to ensure adolescent girls and young women receive meaningful sexual and reproductive health rights support.
The report titled Adolescent Empowerment at a scale: Successes and challenges of an evidence-based approach to young women’s programming in Africa was launched on February 15, 2023, at a BRAC and the United Nations Population Fund (UNFPA) jointly hosted event. The report was written with the support of the Spotlight Initiative, an UN-led, multi-partner initiative that aims to respond to and eliminate violence against women and girls, with a particular focus on family and intimate partner violence, sexual and gender-based violence, and harmful practices.
The history of BRAC’s Empowerment and Livelihood Program (ELA), which was designed to provide sexual and reproductive health education and livelihood training to adolescent girls and young women, is covered in the report. The program was launched in Uganda in 2006 and has since been implemented in Sierra Leone, South Sudan, and Liberia. During the program’s peak from 2013 to 2015, BRAC hosted over 1800 clubs with over 80,000 members.
“The reason that we partnered with BRAC, have partnered with them in the field… is because of the incredible work that they do in this very efficient, kind of way,” said moderator Satvika Chalasani, a Technical Specialist for UNFPA who oversees programs for adolescent girls and ending child marriage.
BRAC’s report Adolescent Empowerment at a scale: Successes and challenges of an evidence-based approach to young women’s programming in Africa talks about its successes and also the need to change programs to ensure their success in a changing society. Credit: BRAC
Chalasani observed that BRAC had gotten to tens of thousands of women on the African continent through their program, Empowerment, and Livelihood for Adolescents, and it was important to learn from their experiences of 15 years in the field.
Willibald Zeck, UNFPA’s Chief of Sexual and Reproductive Health and Rights, also noted BRAC’s record with youth empowerment programs in his opening remarks while adding that demographic changes in certain regions have influenced how such programs must be designed and implemented. It is estimated that over 60% of Africa’s population is under 25.
“As you know, in UNFPA, we really work across the continuum of sexual reproductive health and rights… And we see in certain regions around the globe the new demographics that are showing that there will be more adolescents in the population, but especially on the African continent. Which is a great opportunity in so many ways, but it also brings more challenges.”
Sarah Tofte, a research and policy consultant, and the report’s primary author, presented her findings, breaking down the program’s initial model and implementation and its eventual reset and adaptations.
The report includes findings from academic evaluations conducted by experts, randomized control trials (RCTs) conducted in the regions where ELA programs were hosted, and nearly 100 field interviews with participants and ELA staff.
The findings reveal an overall positive reception and impact on participants and their communities.
Tofte, the co-founder of Understory Consulting, a research and policy consulting firm, noted that the interviewees reported a greater, newfound sense of self through the ELA program, which they connected to making well-informed decisions and contributing productively to the community.
“So based on these positive academic results, and then what I was hearing from field interviews and what participants have been saying over many years, ELA really became a model for other adolescent and youth empowerment programming around the globe, including at the World Bank and at USAID.”
As the report explains, implementation challenges would surface as the program continued. Tofte, the co-founder, noted that while the program’s initial results had been positive, it had slowly ceased to achieve its intended impact.
“By 2017, anecdotal reports had emerged within BRAC about lagging performance of ELA clubs in several countries, including drops in attendance and gaps in the delivery of programming,” she said.
The decline in the program quality and the resulting challenge of sustaining the program over long periods of time also made it difficult to secure funding that would have gone toward addressing the decline. The program had become repetitive for some participants and staff, and issues of deeper community engagement had presented a hurdle for the program’s success.
In 2020, ELA would undergo a “reset” significantly through making fundamental and necessary changes to the curriculum. This would not only update the discussions on reproductive health and livelihood training but would make it more relevant to the economic and social circumstances of the girls they were intended for – while placing more emphasis on providing vocational and livelihood training and financial literacy. Other changes to the curriculum included adjusting the weekly ELA club meetings to optimize engagement and a new graduation model for students to leave the program after one year of completion. The resets were applied at a reduced scale to approximately 140 clubs in the countries where ELA programs were already present.
“Early feedback from this curriculum revamp from the participants suggest that the new curriculum is well received by participants and is driving a positive outcome in attendance and program impact,” Tofte said.
The ELA program adjustments are critical to modernizing the curriculum. What should be of note were the considerations taken to improve community engagement.
“Another big focus of the reset was to deepen community engagement. Prior, a lack of formalized mechanisms for community engagement resulted in some pushback at times from parents of community members who may not have fully bought into the ELA model,” Tofte said. She added that in some cases, the pushback was targeted at the sexual and reproductive health components when the content went against community norms around matters such as child marriage and sexual health.
In response, BRAC, through ELA, has taken measures to establish formal channels with community stakeholders and parents of the participants. By directly engaging with the community’s village elders, religious leaders, and other respected community members, ELA staff members can obtain their support before establishing a program. Formal community leadership committees are also formed, working with ELA staff to ensure smooth operations.
Rudo Kayambo, Regional Director of Africa for BRAC International, pointed out how the findings through field research and the trials were able to be synthesized and focused enough that they could be incorporated into the new program structure, which included paying attention to community members and groups that BRAC did not commonly work with in the past.
“One of the DNAs of BRAC is being able to learn and adapt it quickly,” she said. “…We have now managed to integrate all the lessons into a bigger multicultural program, and some of the key lessons were that they need to support the frontline workers.”
When asked to elaborate, Kayambo added that BRAC would provide technical training and the infrastructure to help monitor and use digital technology. “ are the heart of delivering the value of the ELA program and all its components.”
Another significant change to the rollout of the new ELA program was the introduction of sexual and reproductive health programs targeted at adolescent boys. Boys were included in the program partly to fill a gap in youth-empowerment programs that had thus far been only directed at adolescent girls and women. Through a series of RCTs conducted in 50 rural communities, trial programs similar to ELA were conducted with boys and young men, targeting them specifically.
“ the need to also incorporate adolescent boys and young men, because that formalizes our commitment to getting community buy-in,” said Kayambo.
Manisha Shah, a professor of public policy at UCLA who worked with BRAC to conduct the randomized trials, elaborated that the rationale was to include boys since they were already involved in the decisions and issues that girls and women had to contend with when it came to their health.
“Unless we get these boys on board with the agenda, it’s going to be really hard to think about how we improve the outcomes related to female sexual reproductive health,” she said.
A follow-up survey conducted in those communities two years after the trial programs ended revealed a decrease in intimate partner violence between 20 percent and 60 percent, with a “significant change in these boys’ attitude around violence” and an overall more positive reception and understanding of sexual and reproductive health.
“This just proves that we also need to be targeting the other side of the coin, which is the boys and the young men,” Shah said.
The event also showcased how other organizations partnered with BRAC through the ELA program, such as other NGOs like the Bill and Melinda Gates Foundation. The Foundation’s deputy director for women’s empowerment Diva Dhar remarked that it was critical to recognize that adolescents deal with “really important transitions on school to work, to marriage, to financial, economic independence, to employment.”
“ are a very important age group… because that attitudes and norms crystallize at this age and can have long-term implications, including for future generations,” Dhar said.
When looking at women’s economic empowerment, Dhar stated that further causal evidence would be needed to explore the intersections between economic independence and family planning and health outcomes.
For the Gates Foundation, this has involved investing in programs that build up skills and training for girls and women, including non-traditional opportunities that will build empowerment.
The ELA program in Africa is a testament to BRAC’s success as an NGO, given its ability to inspire similarly multifaceted youth-empowerment programs and its model to evolve and improve their work. However, the report makes it clear that this is achievable through the continued support from partners and donors and from fostering community engagement. Only then can the communities’ women and girls be empowered through the knowledge and skills they obtain through the program.
“One of the key findings we are taking from this is that the role of mentors and community assistance are so important,” Kayambo said. “We are creating room for them to engage from an empowered perspective, and building their own agency, to give room for them to engage and build themselves up before they can empower others in the community.”
Universal Health Care priorities in Pakistan have been boosted by free healthcare insurance for the poor. Credit: Ashfaq Yusufzai/IPS
by Ashfaq Yusufzai (peshawar)
Inter Press Service
PESHAWAR, Feb 22 (IPS) – A free health insurance initiative started in Pakistan has benefited poor patients, especially women who have outnumbered men in using the cashless health services under the Sehat Card Plus programme.
“The initiative is in line with the ICPD25 Programme of Action, under which 4.5 million people have received free services, with 62 percent of them women. In the last three years, we have been able to cut down maternal mortality rate from 186 deaths per 100,000 live births to 172,” Dr Muhammad Riaz Tanoli, CEO of the Sehat Card Plus (SCP), told IPS.
The International Conference on Population and Development (ICPD) held in Nairobi in 2019 set a programme of action aimed at empowering women and girls. The SCP aims to ensure Pakistan meets the 2030 deadline for sustainable development goals for universal health and women.
So far, USD 80 million have been spent on treating patients at 1,100 hospitals across the country.
Shaheen Begum, a resident of Peshawar, is thankful to former Prime Minister Imran Khan, who launched the programme and said that her sister had died of delivery-related complication years ago because they didn’t have money to get quality treatment. She was lucky to undergo a caesarean section at one of the city’s top private hospitals on SCP, and she and her newborn baby are in good health.
“Since my first-month pregnancy, I have been getting diagnostic services free of cost. Two days before delivery, I was admitted because of complications, and doctors performed a caesarean operation,” Begum, 26, a housewife, said.
Pakistanis living abroad with chronic ailments return to the country for treatment. Muhammad Kashif, 55, recently arrived from Malaysia to undergo liver transplant surgery.
Kashif said that the cost of a liver transplant in Malaysia was USD 7,000. Not only was it beyond his reach, but he would have had to call relatives to Malaysia to donate a liver. That would have been impossible, he said in an interview with IPS.
“One of my friends called me and asked to come back and get the surgery free of cost. I came to my native Khyber Pakhtunkhwa province in November last year, and next month, my transplant was done at one of the country’s premier hospitals,” he said.
Like Kashif, Mushtari Gul, a Pakistani nurse working in Saudi Arabia, became extremely sick as her kidneys stopped functioning.
“Initially, I received dialysis for two months, but doctors advised renal transplant that wasn’t possible there due to its cost and donor,” she said.
Gul, 51, is one of the 235 people who received free renal transplants under the SCP. She said it wasn’t possible without an insurance scheme because its cost was USD 6,500, not affordable even by affluent people.
Pakistan Medical Association (PMA) is appreciative of the scheme. “It is an unprecedented programme where the people are able to get services in expensive hospitals. Most patients who couldn’t afford heart surgeries are among the beneficiaries,” PMA’s Secretary, Dr Qaisar Sajjad, told IPS.
PMA has been asking the government to ensure World Health Organization’s aim for Universal Health Coverage is delivered, and this was a step in that direction, Dr Qaisar said.
Public health specialist Dr Fayyaz Shah told IPS that the system has been very good. Unlike the health insurance schemes in developed countries where people deposit annual premiums, here, the government pays the insurance company without charging people.
Before the programme’s launch, the infant mortality rate was 41 per 1,000 live births, which has now come down to 35. Shah elaborated that other health indicators also show improvement as poor people receive timely treatment.
Patients are getting free services for renal and liver transplants and major ailments and procedures, including cancers, surgeries, cardiac diseases, hernia, cataracts, gynaecology, eye, ear, nose and throat and other diseases.
The major beneficiaries are women and children, followed by cancer, heart, dialysis and people with urinary and diabetic problems, he said.
Local gynaecologist Dr Naseem Akhtar terms the programme a blessing for women. Ever since the start of the programme, there has been a drastic decline in mortality among women for pregnancy-related complications.
“Our staff also work harder because they get extra financial incentives from the funds generated from SCP. The patients in hospitals also get free medicines and diagnostic services,” she said.
At the end of every month, we send patients’ details and expenses to the government, and the payment is made within a week. The state-run insurance company is implementing the programme on behalf of the government, which has proved beneficial both for patients and healthcare providers, she said.
A senior nurse, Sania Ali, at a local hospital, said her monthly salary is $200, but she earns $300 additional from the patients undergoing treatment on SCP.
“Our doctors, nurses and paramedical staff want the mechanism to continue as it was a big source of their extra income they received in addition to their fixed salaries,” he said.
“This system has not only helped the poor patients but is also a big source of income for private hospitals. We are extremely busy dealing with patients, and our staff is working round-the-clock to operate on more patients and get more money,” said Dr Shah Raj, a public health physician. She said that each family is entitled to $4,500 per year from the programme. In case of liver and kidney transplants, the patients’ benefits are around $20,000, she said.
The ageing of populations poses mounting challenges for governments that will require changes in national policy priorities, country institutions and social arrangements. Credit: Maricel Sequeira/IPS
Opinion by Joseph Chamie (portland, usa)
Inter Press Service
PORTLAND, USA, Feb 21 (IPS) – Fear of population ageing is all over the news media and in government offices of country capitals worldwide. Planet Earth is becoming “planet ageing”.
Government officials, business leaders, economists, healthcare providers, social organizations, political commentators and others are increasingly ringing alarm bells over the menacing demographic ageing of populations.
Adding to those alarm bells is the 2022 Japanese film, Plan 75, presented in May at the annual Cannes Film Festival. That dystopian film describes a government program that encourages senior citizens to be euthanized to remedy the burdens of an aged Japanese society.
More recently, a Yale University assistant professor of economics reportedly suggested that to address Japan’s demographic ageing, elderly Japanese people should commit “mass suicide”. After raising objections in Japan and elsewhere, he subsequently explained that his suggestion was taken out of context. He explained that his remark was intended to address a growing effort to revamp Japan’s age-based hierarchies and make room for younger generations in leadership positions in business and politics.
Mainstream media regularly reports that government expenditures on retirement and healthcare benefits for the elderly are outpacing tax revenues. Also, many governments are reportedly struggling to find the money to support retirees. Furthermore, current trends, unless they are reversed, indicate that the growing numbers of elderly people on the planet pose a challenge for governments to provide the needed care for them.
People have taken to the streets to protest government proposals to address population ageing by making changes to benefits and official retirement ages. In France people have taken to the streets to protest the government’s intention to raise the current age of 62 years to receive government benefits.
Similarly in China, retirees and their supporters are protesting government proposed cuts in benefits for the elderly. And fearing public backlash at the voting booth, elected government officials in the United States are bending over backwards in their assurances, retreating from possible program cuts, and promising that they “won’t touch” Social Security or Medicare.
The ageing of populations should not really come as a surprise to government officials and their many economic and political advisors and aides.
For decades demographers and many others have been writing articles, publishing books, giving presentations, and advising government officials and others about the demographic ageing of populations resulting from the continued decline in fertility rates and increased life expectancy.
Nevertheless, despite those considerable efforts and clear communication about population ageing, governments have not been paying enough attention.
Apparently, governments mistakenly came to believe that the demographic realities of population ageing could simply be ignored because those realities were largely academic matters as well as concerns for the distant future. In fact, however, those realities were neither largely academic nor concerns for the distant future.
Over the past half century, the median age of the world’s population has increased to 30 years in 2020 from 20 years in 1970, an increase of 10 years. Many countries have attained median ages in 2020 well above 35 years, such as France at 41 years, South Korea at 43 years, Italy at 46 years and Japan at 48 year.
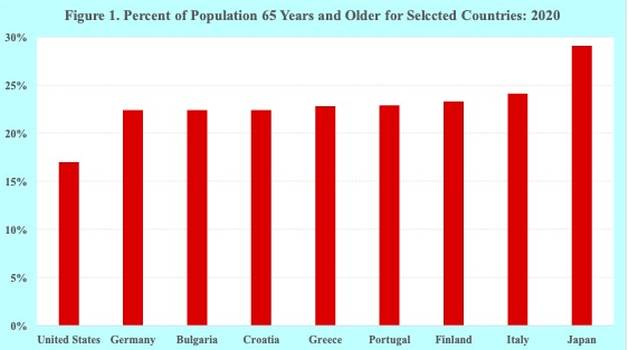
In addition, many countries have seen their elderly population reach unprecedented levels. In the United States, for example, more than 1 in 6, or 17 percent, were 65 or older in 2020. That percentage is relatively low in comparison to many other developed countries. In Italy and Japan, the proportion 65 years and older is 24 and 29 percent, respectively (Figure 1).
Source: United Nations.
The ageing of populations certainly poses mounting challenges for governments as well for the elderly that will require changes in national policy priorities, country institutions and social arrangements.
Among those challenges are needs for financial aid, caregiving and assistance, medical treatment, healthcare and drugs. Such needs are not only increasingly overwhelming many households, but they are also straining government resources and the capacities of institutions to provide care for the elderly.
In addition to the financial costs, governments are wrestling with major policy issues. Population ageing is competing with national priorities that require financial resources, including defense, economy, employment, education, health care, environment and climate.
Population ageing is also raising vexing questions about the proper role of government and the responsibilities of individuals for their personal wellbeing in old age. Those questions continue to roil government legislatures and heighten concerns about retirement and old age healthcare among their citizens.
Much of the public believes that the government should be primarily responsible to cover the financial costs and provide the needed care and support to the elderly, as has generally been the case over the past decades in many countries.
Others, however, contend that it is not the role of the government to be primarily responsible to provide care and support to the elderly. They argue that the elderly themselves and their families should be primarily responsible for covering the costs and providing the needed care, support and assistance for older persons.
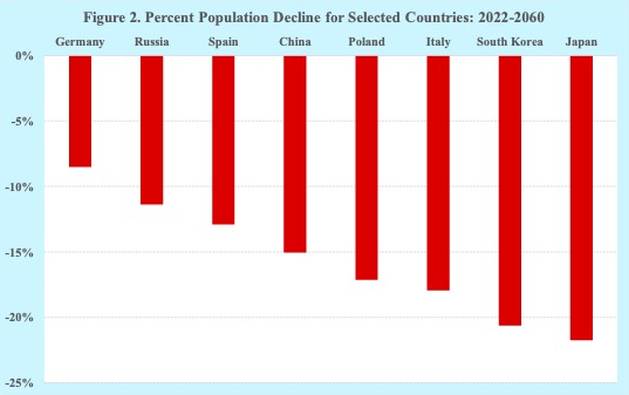
The fear of population ageing is further complicated by population decline. Over the coming years, many countries across the globe are facing declines in the size of their populations due to below replacement fertility rates (Figure 2).
Source: United Nations.
Demographic ageing coupled with population decline and increased human longevity are forcing governments to address mounting financial issues, especially retirement and healthcare benefits. Many government programs for old age benefits are facing insolvency in the near future.
Possible options to address those financial issues include reducing retirement benefits, limiting eligibility, raising the retirement age and increasing taxes. As would be expected, reducing benefits, limiting eligibility and raising retirement ages are unpopular among most of the public. While many are in favor of increased taxes to fund retirement pensions and healthcare for the elderly, businesses and investors are generally opposed to raising taxes.
The consequences of the demographic realities of population ageing are largely unavoidable and need to be addressed. Governments may continue choosing to avoid addressing those consequences. Perhaps they are hoping that if the demographic realities are ignored, they somehow will magically disappear.
Governments need to stop ringing the alarm bells about population ageing. Instead, they need to adapt to the demographic realities of population ageing. In particular, governments need to address the weighty consequences of population ageing by making the admittedly difficult but necessary policy and program decisions regarding official retirement age, pensions benefits, assistance, and healthcare.
Joseph Chamie is a consulting demographer, a former director of the United Nations Population Division and author of numerous publications on population issues, including his recent book, “Population Levels, Trends, and Differentials”.
Everyone loves bread, but it could be a silent killer – and not for the reason you’d think.
Experts warn that an additive not restricted in the US could be making Americans sick. Potassium bromate, the sneaky ingredient in bread that strengthens the dough, is banned from food products in Europe, China and India due to it being a suspected carcinogen.
Erik Millstone, an expert on food additives, claimed that such additives are “almost certainly” causing avoidable illnesses, such as cancer, in Americans.
“There is evidence that it may be toxic to human consumers, that it may even either initiate or promote the development of tumors,” the University of Sussex in England professor told CBS News, adding that European regulations are more restrictive due to food safety diligence.
The Post has reached out to the Food and Drug Administration for comment.
But potassium bromate isn’t the only potentially toxic chemical in our store-bought products. Other substances banned in Europe and allowed in the US are titanium dioxide, brominated vegetable oil, azodicarbonamide and propylparaben.
Additives and chemicals used in American products are advised against in other countries, such as Europe, over health concerns.Getty Images/iStockphoto
Last year, a consumer sued Mars, Inc., over complaints that Skittles contained titanium dioxide, which is used to enhance color. While the lawsuit was dismissed, there have been studies that question the chemical’s safety.
According to Healthline, titanium dioxide is considered safe in the US to be used in food, due to its limited amounts. Additionally, the chemical is used in food packaging, sunscreen and cosmetics, which a 2019 study concluded does “not present any health risk when applied on the skin.”
Brominated vegetable oil is also one of the additives banned across the pond but allowed in American markets. According to the Chicago Tribune, it’s the reason tourists won’t find Mountain Dew in Europe.
Potassium bromate, which is found in bread as a dough strengthener, is one of the additives used in the US that is not considered safe in other places.Shutterstock
Health concerns are centered around one of its components, bromine, due to its ability to irritate the skin and mucous membranes, according to the Mayo Clinic. However, symptoms – such as memory loss and skin and nerve issues – typically occur in soda enthusiasts who guzzle more than 2 liters a day.
Millstone said that many Americans are probably unaware of the chemicals they’re exposed to daily, especially in their own pantries.
“They probably just think, ‘Well, if it’s available or it’s in the store, it’s probably fine,’” he said.
The FDA told CBS News in a statement that they are always reviewing the safety of food and any new information that surfaces. However, they noted that potassium bromate, when used correctly, becomes harmless during the food production process, although it’s not guaranteed that all of the chemical will convert to an innocuous substance.
Earlier this month, a new study suggested that the colorful chemicals used in popular food dyes could have adverse health effects on consumers’ guts. Researchers from Cornell and Binghamton University found that common coloring agents can wreak havoc on the digestive tract.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.