ROME, Jun 03 (IPS) – Developing countries are facing a combination of crises that are unprecedented in recent times. Over the last three years they have had to face the COVID-19 crisis, the food crisis, the energy crisis, the climate change crisis, the debt crisis and, on top of all this, a global recession. The crises have overlapped, and each has added to the problems created by the previous ones.
Daud KhanMuch of the “fault” for these crises lies with the big countries – their desire for geo-political domination, the continued emission of GHGs, the tight money policy of recent months.
There are strong calls for increased aid flows and debt relief, as well as special funds for the countries most affected by high prices, debt burdens or climate change. These actions, much of which will be funded by the developed countries, are needed and necessary to avoid widespread suffering, political turbulence and increased migratory flows.
But these short term actions will not solve underlying problems. There is a need for new thinking; for paradigm shifts; and for new directions by developing countries. So what needs to be done?
Most importantly and most urgently, there needs to be a reform of food systems. Food systems have already shown incredible resilience by coping with COVID related lockdowns, and with the large reverse migrations that took place from urban to rural areas as people lost jobs and incomes. But new directions are needed for food systems to take on the current challenges. Actions are needed in four areas.
• First – developing countries need to reduce their dependence on rice, maize and wheat, three crops which account for half of all calories consumed. For many counties agro-climatic conditions are not suitable for these crops and there is a high reliance on imports. This import reliance has been exacerbated by rapid urbanization that has raised the demand for easily-prepared, convenience food. But there are hundreds, if not thousands of indigenous products – cereals, oilseeds and crops and livestock products that have been ignored by policy makers, researchers and Government extension services. This needs to change.
• Second – food production systems must make increased use of Green Technologies, technologies that are much less reliant on purchased inputs in particular pesticides and chemical fertilizers. Such improved techniques, many of which have been already tried and tested, include integrated pest management, improved crop rotation and multi-cropping, greater use of nitrogen-fixing crops, zero-tillage and mulching. These techniques that make much more intelligent use of the complex interaction between soil, plants, plant residues and livestock waste.
• Third – value chains need to be shortened with monopolies and restrictive practices by traders and middlemen reduced. Progress was made in this regard during the COVID crisis, mainly through greater use of ICT, but this needs to be followed through much more strongly.
• Finally, social safety nets need to be strengthened. Governments cannot cushion the entire population from price increases but does have a responsibility to ensure that children and vulnerable groups are cushioned.
Next in terms of urgency is the energy crisis. A large part of the import bill of many developing countries comprises oil and gas. Reducing this dependence is now more urgent than ever. There are two complementary actions needed:
• First – there has to be a major drive towards increasing production of renewable energy – particularly solar energy. With falling prices of panels, solar energy is now the cheapest form of energy and most developing countries have plenty of space and sunshine.
• Second – solar or wind energy needs to be complemented with other forms of energy that can meet base needs. The most suitable for doing this is through greater use of nuclear energy which, with today’s fourth generation technology, is much safer and less polluting than it used to be. Given high investments costs, as well as the difficulties in setting up suitable regulatory, oversight and contingency systems, smaller countries may need to work jointly to create such nuclear power facilities.
The debt crisis has created a large and growing risk of defaults with the poorest being the most vulnerable. Already in 2019, almost half of low-income and least developed countries (LDCs) were assessed as being at high risk of external debt distress or already in debt distress. Since then, the external debts of developing country have continued to rise and are eating up a growing proportion of export earnings. And this was before the present interest rate hike. Most debt was taken when real interest rate (corrected for perceived risk) were close to zero.
• In addition to ongoing discussions on debt forgiveness, there has to be a discussion between creditors and debtors on repayments especially on interest payments. The burden of the unexpected rise in interest rate needs to be a shared burden.
Finally, developing countries need to find ways to cushion themselves against the recessionary effects of slowing growth world trade. In the current system, global trade flows are dominated by USA, China and Europe.
• In order to break their dependence on these large economies, developing countries need to work to create regional and bilateral trade agreements. Such trade agreements may not be easy. However, the crisis has created conditions where out-of-the-box thinking is essential and cultural and political barriers to regional trade – such as those which limit trade between India and Pakistan – need to be overcome.
Daud Khan works as consultant and advisor for various Governments and international agencies. He has degrees in Economics from the LSE and Oxford – where he was a Rhodes Scholar; and a degree in Environmental Management from the Imperial College of Science and Technology. He lives partly in Italy and partly in Pakistan.
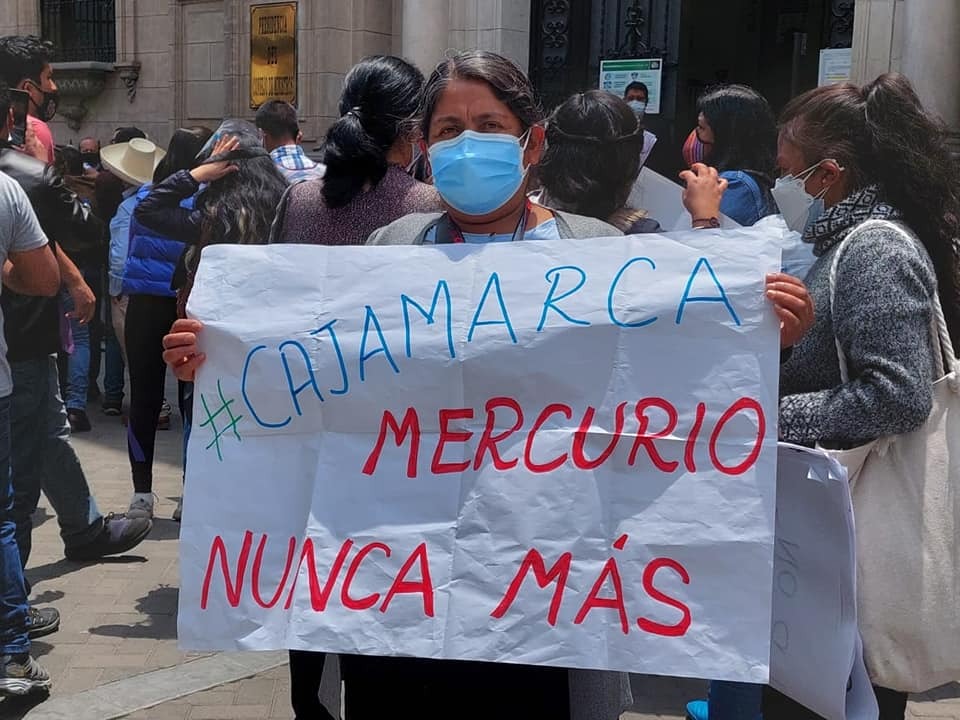
Juana Martínez takes part in an October 2021 protest in Lima organized by the platform of people affected by heavy metals in front of Congress, holding a sign that reads: “Cajamarca. Mercury Never Again”. She was 29 years old when the mercury spill occurred in her town, Choropampa, in Peru’s northern Andes highlands. Several of her relatives have since died from the effects of the heavy metal and one of her sisters became sterile. CREDIT: Courtesy of Milagros Pérez
by Mariela Jara (lima)
Inter Press Service
LIMA, Jun 03 (IPS) – “We are not asking for money, but for our health, for a dignified life,” is the cry of the people of Choropampa, which lawyer Milagros Pérez continually hears 22 years after the environmental disaster that occurred in this town in the department of Cajamarca, in Peru´s northern Andes highlands, on the afternoon of Jun. 2, 2000.
On that day, a Yanacocha Mining company truck spilled 150 kilograms of mercury on its way to Lima, the capital, leaving a glowing trail for about 40 kilometers on the road that crosses Choropampa, a town of 2,700 people located at an altitude of almost 3,000 meters.
The company, 95 percent of which is owned by a U.S. corporation, set up shop there in 1993, 48 kilometers north of the city of Cajamarca, where it operates between 3,400 and 4,200 meters above sea level. Yanacocha (black lagoon in the Quechua indigenous language) is considered the largest gold mine in South America and the second largest in the world, although its production is declining.
Children and most of the population started collecting the shiny droplets scattered on the ground and in the following days, responding to a call from the mining company that announced that it would purchase the material, they picked it up with their own hands, unaware of its high toxicity and that this exposure would affect them for life.
Before the disaster, the town was known for its varied agricultural production which, together with trade and livestock, allowed the impoverished inhabitants of Choropampa to get by as subsistence farmers.
But their poverty grew after the mercury spill, in the face of the indifference of the authorities and the mining company, which never acknowledged the magnitude of the damage caused.
The Choropampa road, now paved, where a truck of a large gold mining company spilled mercury on Jun. 2, 2000, affecting this small town in the department of Cajamarca, in Peru’s northern Andes highlands. The only change since then has been the paving of the road. CREDIT: Grufides
Violated rights
A report, also from the year 2000, by the Ombudsperson’s Office concluded that of the total mercury spilled, 49.1 kilos were recovered, while 17.4 remained in the soil, 21.2 evaporated, and the whereabouts of 63.3 were not identified.
The autonomous government agency also questioned the actions of the authorities and the mining company, referring for example to the extrajudicial agreements they reached with some of the affected local residents, which included clauses prohibiting them from filing any complaint or lawsuit against the company, and which “violate the rights to due process and effective judicial protection of those affected.”
Twenty-two years after the incident, Choropampa’s demands for reparations and access to justice are still being ignored. Pérez, a lawyer with the non-governmental Information and Intervention Group for Sustainable Development (Grufides), based in Cajamarca, said in an interview with IPS that the effects on the local territory and people’s health are evident.
She explained that despite the attempt to hush up the incident, it received enough attention that then president Alberto Fujimori (1990-2000) was forced to promise “an investigation, punishment and reparations” – although these did not happen.
Against a background of poverty and lack of opportunities, the mining company took advantage of the local residents’ goodwill and reached compensation agreements with some of them in exchange for their silence. There were also collective reparation agreements such as the construction of a town square, but nothing that actually contributed to remedying and addressing the damage caused to the people, say experts and activists.
For instance, the mining company committed to a private health plan for the people who were affected by the disaster, but it ended up being “a sham,” she said.
“They give them pills for the pain and nothing more, to people affected by mercury, while every day it becomes more difficult for them to support their families as they suffer terrible loss of vision, decalcification, bone malformations, and permanent skin irritations, which make it impossible for them to work their land and lead the lives they had before,” said Pérez.
Lawyer Milagros Pérez, who is dedicated to fighting for the reparations demanded by the population of Choropampa after a mercury spill in 2000 by the Yanacocha Mining Company in this town in the northern Andean department of Cajamarca, Peru, which caused irreversible damage to their health and lives. CREDIT: Mariela Jara/IPS
Women, affected in very specific ways
The Grufides attorney stated that there is also an additional impact that has remained in the dark until now.
“Although the population in general has suffered damage to the corneas, nervous system, digestive system, skin, and bone malformations, we have noticed specific problems in women related to their reproductive capacity, such as premature births, miscarriages, sterility and births of infants with malformations, which have not been investigated,” she said.
Pérez criticized the fact that to date the affected population continues without specialized attention, with access only to a health post with a general practitioner and three nurses, who lack the capacity to deal with the specific ailments caused by contamination with heavy metals such as mercury.
“What the women are experiencing is part of this overall situation, effects that began in the year 2000 after the spill, according to the testimonies we have been collecting. But they need a specialized health diagnosis, something as basic as that, in order to begin to remedy the damage,” she said from Cajamarca, the capital of the department.
Pérez also mentioned the effects on women’s mental health and their role as caregivers, as a collateral aspect of this tragedy that has not yet been documented.
She cited the example of Juana Martínez, who is known for her defense of the rights of the local population and who for this reason has been threatened and slandered by unidentified persons.
“I tell her, Juanita, you don’t die because everyone needs you, that keeps you alive; because as a result of the contamination, her sister, her mother-in-law and her sister-in-law all died. There is a chain of contamination, the problem is much bigger and it affects different generations, but they don’t want to study it,” she said.
IPS tried to contact Martínez, but was unable to do so because she lives in a remote area far from the town, where there is no cell phone signal.
Denisse Chávez is an ecofeminist activist and member of the team promoting the Third International Tribunal for Justice and Defense of the Rights of Pan-Amazonian-Andean Women, to be held Jul. 30 in the city of Belem do Pará, Brazil, where the case of the women of Choropampa, whose health was affected by mercury contamination in 2000, will be presented. CREDIT: Mariela Jara/IPS
Getting their voices heard in an international ethical tribunal
Denisse Chávez, an ecofeminist activist, told IPS that the case of the women of Choropampa affected by the mercury spill will be among those presented at the Third International Tribunal for Justice and Defense of the Rights of Pan-Amazonian-Andean Women, to be held Jul. 30, 2022, in the city of Belem do Pará in Brazil’s Amazon region.
The tribunal is one of the emblematic activities to take place within the framework of the 10th Pan-Amazonian Social Forum, which under the slogan “weaving hope in the Amazon” will bring together for four days some 5,000 people from different countries of the Amazon basin interested in coordinating actions in defense of nature and the Amazon rainforest.
Chávez, a member of the group organizing the tribunal, which also includes feminist and human rights activists from Brazil, Ecuador, Colombia and Uruguay, denounced that the Peruvian State has failed to make the company compensate the damage caused to the local population or to make visible the specific impacts on women, in the past 22 years.
“Choropampa is an area far from the city and with a highly vulnerable population, with high rates of poverty and illiteracy. In more than two decades no government has been interested in solving the problems while the mining company continues to offer solutions on an individual basis, which is violent since money is offered so that people do not talk,” she added.
She said the tribunal will bring the case international visibility, like others from Brazil, Colombia and Ecuador, which “have in common the impact caused by extractive economic activities on the lives of our peoples and especially on the bodies of women, which is still not taken into account or discussed.”
The ethical, symbolic tribunal will issue a judgment specifying the violations of women’s human rights and the obligations incumbent upon States and corporate actors.
Chávez said the document would be sent to the Peruvian authorities, both in Cajamarca and at the national level. “We cannot allow impunity in the Choropampa case; we will continue to keep the memory of what happened alive,” she said.
Pérez pointed out that the government’s decision was the result of pressure from civil society and groups affected by heavy metals. But Choropampa has not been included in this first stage, despite the lasting impact on its population and soils.
“It is supposed to expand gradually but we will be closely watching the decisions that are taken because a protocol of attention and budgets for diagnostics must be elaborated,” she said.
Juana Martínez takes part in an October 2021 protest in Lima organized by the platform of people affected by heavy metals in front of Congress, holding a sign that reads: “Cajamarca.
“Investigations are ongoing, but the sudden appearance of monkeypox in many countries at the same time suggests there may have been undetected transmission for some time,” Tedros Adhanom Ghebreyesus told journalists at WHO’s Geneva headquarters.
Be vigilant
With most reported cases having been among sexual encounters between men, those communities are working to inform their members of risks and preventative action that can be taken.
“But all of us must work hard to fight stigma, which is not just wrong, it could also prevent infected individuals from seeking care, making it harder to stop transmission,” warned the WHO chief, urging affected countries to widen their surveillance to the broader community.
Anyone risks infection if they have close physical contact with someone who has Monkeypox.
Tedros noted that as the situation is evolving, WHO expects more cases to be found.
“It’s important to remember that generally, Monkeypox symptoms resolve on their own, but can be severe in some cases,” he added.
WHO continues to receive updates on the status of ongoing Monkeypox outbreaks in African countries where the disease is endemic.
The top WHO official outlined his priorities to provide accurate information to those most at-risk; prevent further spread among those at high risk; protect frontline health workers; and advance “our understanding” of the disease.
Monkeypox lesions often appear on the palms of hands.
COVID trends
Meanwhile, as reported COVID-19 cases and deaths continue to decline globally, Tedros cautioned that this may be the result of reduced testing throughout many countries.
But in several regions in the Americas, cases, and deaths are surging, while there are increasing fatalities in the Western Pacific region and Africa.
“Once again, the pandemic is not over. We continue to call on all countries to maintain testing and sequencing services, to give us a clearer picture of where the virus is spreading, and how it’s changing,” said the WHO chief.
“We call on all countries to vaccinate all health workers, older people and other at-risk groups”.
Care in Ukraine
With the war in Ukraine taking a heavy toll on the country’s health system, WHO has increased its presence in the country and in States hosting displaced people – as the number of healthcare attacks continues to rise.
“More than 6 million people remain under siege by Ethiopian and Eritrean forces, after more than 18 months. Although some food is being delivered, it’s not enough, and basic services remain unavailable”-@DrTedros#Tigrayhttps://t.co/kxUx2eG4Az
— World Health Organization (WHO) (@WHO) June 1, 2022
“As of yesterday, WHO has verified 269 attacks on health in Ukraine, killing 76 people and injuring 59,” Tedros said.
“Healthcare must never be a target,” he added, calling again on Russia to end the war.
Rippling effect of war
Russia’s invasion has disrupted global food supplies and exacerbated the risk of famine around the world, he said.
As the Horn of Africa suffers one of its worst droughts in recent history, the rising risk of famine and malnutrition is severely affecting an estimated 15 to 20 million people in Kenya, Somalia, and Ethiopia, as well as affecting populations in Djibouti, Eritrea, Uganda, South Sudan and Sudan.
The WHO chief said there were tens of thousands of families forced to leave home in search of food, water and pasture, which is leading to mass displacement and a lack of safe drinking water, hygiene and sanitation – further heightening health risks.
“This is especially worrying in an already under-immunized population with little access to health services,” pointed out the WHO chief.
At the same time, more than six million people remain under siege by Ethiopian and Eritrean forces in Tigray.
As the region is sealed, not enough food is being delivered and basic services remain unavailable.
“WHO is doing its best to help, but the only solution to this inhumane situation – as in Ukraine – is peace,” he underscored.
WHO business
Turning to the first in-person World Health Assembly since the COVID-19 pandemic began – which ended on Saturday – Tedros drew attention to the adopted “landmark resolution to increase assessed contributions” to a target of 50 per cent of WHO’s base budget by the end of the decade, up from today’s 16 per cent.
“This change will give WHO the flexibility and predictability to plan for long-term programming in countries, and to attract and retain the people we need to deliver those programmes,” he said.
Other Assembly decisions strengthens WHO’s preparedness and response to health emergencies.
ROME, Jun 01 (IPS) – Developing countries – in Africa, in Asia, in Latin America and in the Middle East – are facing a combination of crises that are unprecedented in recent times. Over the last three years they have had to face the COVID-19 crisis, the food crisis, the energy crisis, the climate change crisis, the debt crisis and, on top of all this, a global recession. The crises have overlapped, and each has added to the problems created by the previous ones.
Daud KhanFirst among the crises relates to food – the most basic of human needs. Even before the events in Ukraine there were shortages and uncertainties. International food prices rose by 40% over their level of 2020 – with increases of almost 90% in the price of vegetable oil – pushing up domestic food prices in both importing and exporting countries, and driving millions towards food insecurity. And then came the Ukraine crisis; and price of cereals and cooking oils spiked yet again – up 20% for cereal and 30% for vegetable oils.
And it is not just an issue of prices. Supplies are hard to come by. In April 2022 Ukraine exported only 1 million tons of grain as opposed to a normal export volume of 5 million tons and Indonesia banned exports of palm oil. On top of this came climate change. Low rainfall and drought-like conditions have also affected production in several major wheat exporting countries such as France and the USA. Scorching temperatures across northern India and Pakistan have reduced wheat output by 20% and in response, India has now banned exports of wheat.
The second crisis relates to the price of energy. Energy prices before the Ukraine crisis has risen 75% in twelve months and another 25% since then. This has raised costs of transport, manufacturing and services. Prices of natural gas, which drives the prices of urea fertilizer, rose by over 140% and this will impact plantings, yields and output of food crops in coming years. The prices of phosphate fertilizers have also risen – by over 200% the last year – with about a third of the increase coming since January 2022, mainly as a result of disruption of supplies.
The next punch in the belly for developing countries came from interest rates increases. Developing country debt has boomed in over the past decades years, fueled by the easy availability of savings and real interest rates of virtually zero. With rising inflation, the US Federal Reserve Board has hiked up interest rates. This has not only increased interest payments but also the value of the US$ in which much developing country debt is denominated. This is making debt servicing vastly more expensive and balance of payments problems are looming large for many countries. Higher debt servicing is also putting pressure on Government budgets and is resulting in large cuts in development and social spending.
And we are not finished yet. Global GDP and trade are slowing down. This reflects the recessionary cocktail of high energy prices, supply bottlenecks, rising interest rates and political uncertainties around the globe, as well as COVID-related lockdowns in China.
This perfect storm is mostly the result of the policies of the big economies – the ongoing US/Russia/China rivalry; rapid globalization followed by the strict COVID-related lockdowns; and easy monetary policies which first pumped in huge sums of money into the economies and are now raising interest rates to rein in inflation. Climate change has much to do with large and continued emission of GHGs, the bulk of which comes from the big economies, including China. And now, speculative capital, mostly originating in the developed world, is further aggravating the situation in food, fuel and other commodity markets.
But the interlinked nature of the globalized world implies that in relative terms the financial and human burden of these actions falls heaviest on developing countries. After all it is one thing for food and energy prices to rise, or for GDP growth to slow in rich countries such as the USA, Europe and Australia, or even in China. In these countries living standards are high, infrastructure and services are well developed, and often well designed social safety nets are in place. It is quite different in developing countries, where large numbers continue to live with poverty and hunger; where basic services such as education, health and clean drinking water are scarce; and those facing old age, illness or loss of earnings can only rely on the goodwill of friends or family.
There is, quite rightly, much concern about the situation. Several high level meetings have been convened, including by the UN, and there are strong calls for increased aid flows and debt relief, as well as for the creation of special funds for the countries most affected by high prices, debt burdens or climate change. These actions are needed and necessary to avoid widespread suffering, political turbulence and increased migratory flows. And the developed countries will likely bear most of the financial burden of these measures.
But many of the measures, even if implemented, are short term palliatives and will not solve underlying problems. Moreover, developing countries cannot continue to rely indefinitely on goodwill and charity. The risk of doing this became very clear during the COVID crisis where little of the vaccines available and none of the vaccine production technology were shared.
However, times of crisis also create opportunities. There is a need for new thinking and for paradigm shifts in developing countries but also for Governments to undertake reforms that they have been postponing for years, if not decades, due to fears that such reforms would hurt vested interests and national elites. It is now time to act bravely.
Part two of this article will discuss some of the concrete measure that developing countries could take to address the various crises.
Daud Khan works as consultant and advisor for various Governments and international agencies. He has degrees in Economics from the LSE and Oxford – where he was a Rhodes Scholar; and a degree in Environmental Management from the Imperial College of Science and Technology. He lives partly in Italy and partly in Pakistan.
The UN agency revealed that the tobacco industry costs the world more than eight million human lives every year. As well as the human costs, 600 million trees, 200,000 hectares of land, 22 billion tonnes of water, and 84 million tonnes of CO2 are used in the production of tobacco.
Most of the environmental cost falls on low-and-middle-income countries, where water and farmland are used to grow tobacco plants, instead of for food production, which is often desperately needed.
The WHO report “Tobacco: Poisoning our planet” highlights that the industry’s carbon footprint from production, processing and transporting tobacco is equivalent to one-fifth of the CO2 produced by the commercial airline industry each year, further contributing to global warming.
Unsplash/Lex Guerra
Tobacco use is one of the leading preventable causes of death.
Trillions of filters pollute the planet
“Tobacco products are the most littered item on the planet, containing over 7,000 toxic chemicals, which leech into our environment when discarded”, said Dr Ruediger Krech, Director of Health Promotion at WHO. “Roughly 4.5 trillion cigarette filters pollute our oceans, rivers, city sidewalks, parks, soil and beaches every year”.
Products like cigarettes, smokeless tobacco and e-cigarettes also add to the build-up of plastic pollution. Cigarette filters contain microplastics and make up the second-highest form of plastic pollution worldwide.
The WHO is calling for policy-makers to treat cigarette filters the same as any other single-use plastic, and consider banning them, to protect public health and the environment: despite tobacco industry marketing, there is no evidence that filters have any proven health benefits.
Farmers processing their tobacco to sell it at he market in Mzingo Village, Malawi.
Make the polluter pay
The costs of cleaning up littered tobacco products fall on taxpayers, rather than the industry creating the problem. Each year, this costs China roughly $2.6 billion and India roughly $766 million. The cost for Brazil and Germany come in at over $200 million.
However, countries like France and Spain and cities like San Francisco, California in the USA are taking a stand. Following the “polluter pays” principle, they have successfully implemented legislation which makes the tobacco industry responsible for clearing up the pollution it creates.
WHO urges countries and cities to follow this example, as well as give support to tobacco farmers to switch to sustainable crops, implement strong tobacco taxes and offer support services to help people quit tobacco.
Adequate maternal care during pregnancy, childbirth and the postpartum period is essential to curbing the high maternal mortality rates in Latin America, which stopped falling due to women’s health care problems during the COVID pandemic. CREDIT: Government of Tigre / Argentina
by Mario Osava (rio de janeiro)
Inter Press Service
RIO DE JANEIRO, May 28 (IPS) – Brazil had the dubious distinction of champion of maternal mortality in Latin America during the COVID-19 pandemic, with a 77 percent increase in such deaths between 2019 and 2021.
A total of 1,575 women died in childbirth or in the following six weeks in the year prior to the pandemic in Latin America’s largest and most populous country, with a population of 214 million. Two years later the total had climbed to 2,787, according to preliminary data from the Health Ministry’s Mortality Information System.
In Mexico, the second-most populated country in the region, with 129 million inhabitants, the increase was 49 percent, to 1,036 maternal deaths in 2021. And in Peru, a country of 33 million people, the total rose by 63 percent to 493 maternal deaths.
In Colombia, recent data are not available. But authorities acknowledge that in 2021 COVID-19 became the leading cause of maternal deaths, as it was in Mexico.
Brazil is the extreme example of multiple mistakes and of stubborn denialism that led to many avoidable deaths, particularly of pregnant women, according to experts and women’s rights activists on the occasion of the International Day of Action for Women’s Health, celebrated May 28.
A woman takes part in a care program for pregnant women in a low-income area of the northern state of Pará, Brazil. PAHO warned that the disruption of health services caused by COVID drove up maternal mortality rates in Latin America and the Caribbean. CREDIT: UNFPA
Something smells rotten
“Inadequate prenatal and obstetric care,” largely due to inadequate medical training in these areas, is the cause of the tragedy in Brazil, said physician and epidemiologist Daphne Rattner, a professor at the University of Brasilia and president of the Network for the Humanization of Childbirth.
“Hypertensive syndrome is the main cause of death in Brazil, while in the world it is hemorrhage. In other words, there is some failure in a simple diagnosis like hypertension and in managing it during pregnancy and childbirth,” she said in an interview with IPS from Brasilia.
Of the 38,919 maternal deaths between 1996 and 2018 in Brazil, 8,186 were due to hypertension and 5,160 to hemorrhage, according to a Health Ministry report. These are direct obstetric causes, which accounted for just over two-thirds of the deaths. The rest had indirect causes, pre-existing conditions that complicate childbirth, such as diabetes, cancer or heart disease.
An excess of cesarean sections is another factor in mortality. It is “an epidemic” of 1.6 million operations per year, the Health Ministry acknowledges. This is equivalent to about 56 percent of the total number of deliveries. The proportion reaches 85 percent in private hospitals and stands at 40 percent in public services, well above the 10 percent rate recommended by the WHO.
“They don’t practice obstetrics, they practice surgery, they don’t know how to provide clinical care, and the result is more maternal deaths,” Rattner lamented.
And the pandemic made the situation more tragic.
Black women protest to demand respect for their rights in Brazil. Black women are the greatest victims of maternal mortality caused by COVID-19 in the country. They account for almost twice the number of deaths of white mothers, according to a study by the Oswaldo Cruz Foundation, the leading national health research institution. CREDIT: Fernando Frazão / Agência Brasil
The stork doesn’t come anymore
Brazil missed the target of reducing maternal mortality by 75 percent by 2015, from 1990 levels, but it was moving in that direction. The maternal mortality ratio (MMR) per 100,000 live births in the country fell from 143 to 60, a 58 percent drop.
The Stork Network, a government strategy adopted in 2011 to improve assistance to pregnant women and the infrastructure of maternity hospitals, humanize childbirth, ensure family planning and better care for children, helped bring the MMR down.
But COVID-19 and the government’s response to it caused a setback of at least two decades in Brazil’s maternal mortality rate.
Coronavirus killed more than 2,000 pregnant and postpartum women in the last two years and there are at least 383 other deaths from severe acute respiratory syndrome that may have been caused by COVID-19, according to the Feminist Health Network, an activist movement that has been fighting for sexual and reproductive rights since 1991.
The way the government of far-right President Jair Bolsonaro acted “was a maternal genocide, not just a disaster,” said Vania Nequer Soares, a nurse with a PhD in public health who is a member of the Feminist Health Network.
The government’s denialism and its response to the pandemic aggravated mortality in general, which already exceeds 666,000 deaths, as well as maternal mortality. Health authorities took more than a year to recognize that pregnant women were a high-risk group for COVID-19, made it difficult for them to receive intensive care and delayed their vaccination, Soares said.
To make matters worse, they decided to dismantle the Stork Network, whose public policies had promising results, and adopted new rules of “obstetric violence” included in the brand new Maternal and Child Care Network (Rami), which concentrates all power in doctors and hospitals, to the detriment of other actors and dialogue, she told IPS by telephone from Lisbon.
Miriam Toaquiza, a teenage mother, and her newborn daughter, Jennifer, are photographed at a hospital in Ecuador. Latin America is second in the world in teen pregnancy, one of the causes of the high maternal mortality rates in the region. CREDIT: Gonzalo Ortiz/IPS
Undernotification and negligence
But the numbers of maternal deaths are probably higher. Brazil was slow to begin using COVID-19 diagnostic tests and did not test widely. And because clinical identification of the new disease was doubtful, many mothers probably died without the correct diagnosis, especially in the first year of the pandemic, Rattner argued.
A study published this month in the scientific journal The Lancet Regional Health – Americas, with accounts from the families of 25 pregnant women who died of COVID-19, revealed three practices that condemned many women to death on the verge of childbirth.
First, doctors refused to hospitalize or better examine those who complained, for example, of difficulty breathing. They attributed it to late pregnancy and delayed a diagnosis that could have saved at least one life.
In other cases, health centers turned away pregnant women because they were dedicated to the COVID-19 emergency, arguing that they could not accept pregnant women because of the risk of infecting them. And in maternity wards, pregnant women were turned away because of the risk that they could bring in coronavirus and affect other women.
Finally, pregnant women who managed to be accepted in hospitals were denied intensive care, under the argument of protecting the baby’s life. In other words, the choice was made to save the child, to the detriment of the mothers, without consulting the families.
This was confirmed by the fact that all 25 pregnant women died, but 19 babies survived. Four families told the health professionals that they wanted the mother to be saved, even arguing that she could have other children in the future, but this proved to be in vain.
The study by three researchers from the Anis Institute of Bioethics, Human Rights and Gender, based in Brasilia, corroborates the complaint of the Feminist Health Network that 20 percent of the pregnant and postpartum women did not have access to intensive care and 32.3 percent were not put on ventilators.
Women must be given protagonism, so that “they can take ownership of the process of motherhood, including childbirth,” said Ligia Cardieri, a sociologist who is executive coordinator of the Feminist Health Network.
Fewer mechanical interventions, a reduction of c-sections that increase risks, including anesthetics, and greater involvement of nurses and other maternal health actors are other recommendations to avoid so many maternal deaths, she told IPS from Curitiba, capital of the southern state of Paraná.
In other Latin American countries, pregnant women with COVID-19 suffered a similar lack of attention and problems.
Nearly a third of them were not given intensive care or respiratory support during the pandemic, revealed a study of 447 pregnant women from eight countries, including five from South America, two from Central America and one from the Caribbean, according to PAHO data.
Women would rather suffer in silence at work than admit they are struggling with a health condition, new research has revealed.
Around six in 10 women say they wouldn’t feel comfortable discussing topics such as menstrual cramps, smear tests, breast examinations or menopause with a manager.
The poll of 2,000 adults who are biologically female found that 40 percent said this was because it would be too awkward an uncomfortable.
Around 36 percent said they would feel embarrassed, and 22 percent said they would keep quite as they didn’t want to come across as a ‘slacker’ to other.
It’s not just in the workplace where women are keeping tight lipped, as a quarter won’t discuss post-pregnancy issues with family or friends.
The study was commissioned by health and dental plan provider Simplyhealth to spark one million ‘comfortable conversations’ about female health during Women’s Health Month with its campaign #comfyconvos.
Clinical Director, Catherine Rutland, said: “No one should suffer in silence and our survey shows that too many women in the UK are doing just that.
“Whether that is at work, or in their personal life, women are feeling uncomfortable or embarrassed discussing perfectly normal health concerns.
“It’s time we broke down those barriers and banished the taboos.”
The study also found 47 percent of employed respondents didn’t think their bosses would understand health issues specifically affecting their gender.
While 43 percent worried they’ll be viewed as weak, and 47 percent didn’t think their issue would be recognized as an illness.
New research reveals women would rather suffer in silence at work than admit they are struggling with a health condition.Getty Images/iStockphoto
Despite 54 percent having no problem discussing general health conditions, such as the flu, back pain and Covid-19, 43 percent have ‘suffered in silence’ at work while being worried about a female-specific ailment.
Menstrual cramps (33 percent) and menopause (18 percent) are among the issues women have kept to themselves.
While 13 percent have suffered with miscarriage but didn’t tell their employer anything was wrong.
In fact, more than a quarter would keep quiet about miscarriage over fears it would impact their career opportunities or potential pay increases.
It also emerged three in 10 professionals have lied to an employer about why they’ve needed time off work when experiencing a female health issue.
Only one in 10 of those who are going through or have gone through the menopause feel comfortable enough to approach their manager for time off due to symptoms.
In comparison, 40 percent would ask permission to visit the dentist.
Loss of concentration (40 percent), crumbling anxiety (39 percent) and debilitating hot flushes (35 percent) are among some of the menopausal symptoms people admit to hiding at work.
Women’s health issues are also impacting exercise for many, with 44 percent claiming painful menstrual cycles stop them from playing sport or going to the gym.
And 39 percent admitted feelings of shame or embarrassment of their body puts them off exercise or playing sport publicly.
A further 46 percent of women polled via OnePoll are also demonstrating reluctance to have these conversations with their GP, with 45 percent more likely to open-up if they had access to more bespoke health services, more in tune with women’s needs.
Catherine Rutland added: “We’ve have been providing access to healthcare for 150 years, following this insight, we understand that more needs to be done.
“That’s why it is encouraging one million comfortable conversations about women’s health in 2022.”
This story originally appeared on The Sun and was reproduced here with permission.
Nigerians should not be pushing against global COVID-19 vaccine inequity amid widespread looting of the national treasury. Credit: UNICEF/Nahom Tesfaye
Opinion by Ifeanyi Nsofor (abuja)
Inter Press Service
ABUJA, May 24 (IPS) – Nigeria’s accountant-general, the administrative head of the country’s treasury, has been arrested by the Economic and Financial Crimes Commission for allegedly stealing 80 billion naira ($134 million). This is a staggering theft in a country that has an estimated poverty rate of 95 million (48% of the population) and some of the worst health indices in the world.
As a universal health coverage and global health equity advocate, I know that Nigeria’s health system would be stronger and work better by blocking these leakages and channeling the funds to provide universal health coverage for every Nigerian.
Indeed, the stealing of public funds denies millions of people healthcare, which comes with severe health consequences. These include citizens living with chronic debilitating illnesses, loss of productivity, worsening poverty and even death. In our country, about 58,000 women die during pregnancy and childbirth yearly; and 1 in 8 children do not live to witness their 5th birthday. Simply put, corruption is a matter of life and death.
These are five examples of how the missing 80 billion naira could improve the health of Nigerians if rechanneled.
First, 80 billion naira would fund President Muhammadu Buhari’s plan to provide health insurance for 83 million poor Nigerians, as part of his implementation of the new National Health Insurance Authority Act that he recently signed into law.
Further, the missing 80 billion naira is 114 times the 701 million naira budgeted for the defunct National Health Insurance Scheme in 2022. It is unsurprising that the Scheme did not achieve a national health insurance coverage of up to 5% for the past 18 years.
A mandatory health insurance program is a way to achieve universal health coverage for Nigerians because out-of-pocket spending at the point of healthcare pushes people into poverty. Isn’t it ironic that millions of Nigerians are pushed into poverty when they access healthcare and the accountant-general is alleged to have stolen 80 billion naira? This is a classic case of suffering in the midst of plenty.
Second, the stolen 80 billion naira can fund tertiary healthcare for millions of Nigerians who access care at teaching hospitals. Lagos University Teaching Hospital, University of Nigeria Teaching Hospital, University of Ibadan Teaching Hospital, Aminu Kano Teaching Hospital and Jos University teaching Hospital collectively have a budget of 78 billion naira for 2022.
Teaching hospitals do not just provide tertiary healthcare. They also provide primary and secondary healthcare services. In addition, they train medical students and other health professionals. They are also training institutions for doctors specialising to become consultants.
Third, the stolen 80 billion naira is 13 times the 6 billion naira collectively budgeted for National Obstetric Fistula Centres at Abakaliki, Bauchi and Katsina states in 2022. The World Health Organization describes obstetric fistula as an abnormal opening between a woman’s genital tract and her urinary tract or rectum.
It is caused by long obstructed labor and affects more than 2 million young women globally. The abnormal opening leads to leakage of urine and/or faeces from the vagina. Obstetric fistulas destroy the dignity of women. Victims are ostracized, stigmatized and lose economic power. It said that you smell victims before you see them.
That is the huge burden that victims carry. In Nigeria, prevalence of obstetric fistula is 3.2 per 1000 births. There are 13,000 new cases yearly. A review of obstetric fistula in Nigeria showed that the backlog of cases could take 83 years to clear.
In contrast, the stolen 80 billion naira would shorten the time it takes to clear this backlog. I know from my experience as a grantmaker. In 2012, I led the community health initiatives at the TY Danjuma Foundation. A one-year grant of 11 million naira awarded to a grantee in Kano state, northwest Nigeria provided surgical repairs of obstetric fistulas; training of health workers on repair and care of patients; economic empowerment of patients; and advocacy to communities to discourage early marriage and encourage health-facility-based deliveries.
Fourth, the missing 80 billion naira if allocated to the National Primary health Care Development Agency would improve COVID-19 vaccines procurement, distribution and administration in Nigeria. Indeed, that amount is more than 3 times the 24 billion naira budgeted for the NPHCDA in 2022.
So far, Nigeria is mostly depending on the generosity of vaccines donated by rich countries such as the U.S. through the COVAX facility. This is not sustainable. Recent news out of South Africa reveals that Aspen Pharmacare could shut down production of Johnson & Johnson COVID-19 vaccine because African countries are not placing orders as expected.
At a cost of $7.50 per dose of Johnson & Johnson COVID-19 vaccine, $134 million would buy 18 million doses to vaccinate Nigerians and help the country achieve herd immunity as quickly as possible. Nigerians should not be pushing against global COVID-19 vaccine inequity amid widespread looting of the national treasury.
Lastly, the stolen 80 billion naira is 1.5 times the amount budgeted for the 54-billion-naira Basic Health Care Provision Fund. According to the National Primary Health Care Development Agency, the fund is to improve access to primary health care by making provision for routine costs of running primary health centres, and ensure access to health care for all, particularly the poor, by contributing to national productivity. Eighty billion naira increases the number of poor and vulnerable Nigerians who could access healthcare through the Basic Health Care Provision Fund.
Sadly, while still trying to come to terms with the allegation against the accountant-general, there is more news of fraud in Nigeria. A former Managing Director of the Niger Delta Development Commission was arrested for allegedly stealing 47 billion naira. Also, the only female to have served as the speaker of Nigeria’s federal House of Representatives was also arrested for 130 million naira fraud.
These thefts must stop, and the funds should be put where they are most needed: funding healthcare. Without health, we have nothing.
First elected in 2017, his re-election by secret ballot, was confirmed during the 75th World Health Assembly in Geneva. He was the sole candidate.
The vote was the culmination of an election process that began in April 2021 when Member States were invited to submit proposals for candidates for the post of Director-General. The WHO Executive Board, meeting in January of this year, nominated Dr Tedros to stand for a second term.
His re-election was met with wide and loud applause from ministers and others at the Assembly in Geneva. According to news reports he received 155 out of 160 votes cast, although he did not win the support of his native Ethiopia, due to opposing views over the Tigray conflict.
The WHO chief’s new mandate officially commences on 16 August. A Director-General can be re-appointed once, in accordance with World Health Assembly rules and procedures.
‘Humbled and honoured’
In a tweet following the vote, Tedros said that he was “humbled and honoured” by the vote of confidence, adding that he was “deeply grateful for the trust and confidence of Member States.”
“I thank all health workers and my WHO colleagues around the world”, he continued saying he was looking forward to “continuing our journey together.”
In remarks after the vote, he said his re-election was a vote of confidence in the whole WHO adding: “this is for the whole team.”
He acknowledged the pressure and attacks from “many quarters” during the pandemic, saying that despite the insults and attacks, he and the organization always kept an open mind and did not take it personally.
“We have to focus on promoting health…number two, we have to focus on primary healthcare” and thirdly, he cited the importance of emergency preparedness and response, being dependent on the first two priorities.
Transformation
During his first term, Tedros instituted a wide-ranging transformation of the WHO, the agency said in a press release, “aimed at increasing the Organization’s efficiency driving impact at country level to promote healthier lives, protect more people in emergencies and increase equitable access to health.”
Tedros guided WHO’s response to the unprecedented COVID-19 pandemic, where he sometimes faced criticism, most notably, from former United States President, Donald Trump, who took the decision to withdraw the US from the WHO – a move since reversed.
The WHO chief also steered the response to outbreaks of Ebola in the Democratic Republic of the Congo (DRC) and led the agency dealing with the health impacts of multiple other humanitarian crises, most recently the war in Ukraine.
Ministerial career
Before first being appointed WHO Director-General, Dr Tedros served as Minister of Foreign Affairs for Ethiopia between 2012 and 2016 and as Minister of Health prior to that, from 2005.
He had also served as chair of the Board of the Global Fund to Fight AIDS, Tuberculosis and Malaria; as chair of the Roll Back Malaria (RBM) Partnership Board; and as co-chair of the Board of the Partnership for Maternal, Newborn and Child Health.
As of May 21, the World Health Organization (WHO) received reports of 92 laboratory-confirmed cases and 28 suspected cases from 12 countries not endemic for the disease.
Some cases have been identified through sexual health clinics and investigations are ongoing.
The disease could affect anyone
According to WHO, available evidence suggests that those who are most at risk are those who have had close physical contact with someone with monkeypox, and that risk is not limited to men who have sex with men.
UNAIDS urged media, governments, and communities to respond with a rights-based, evidence-based approach that avoids stigma.
“Stigma and blame undermine trust and capacity to respond effectively during outbreaks like this one,” said Matthew Kavanagh, UNAIDS Deputy Executive Director. “Experience shows that stigmatizing rhetoric can quickly disable evidence-based response by stoking cycles of fear, driving people away from health services, impeding efforts to identify cases, and encouraging ineffective, punitive measures”.
Mr Kavanagh highlighted that the agency appreciates the LGBTI community for having led the way in raising awareness of Monkeypox and reiterated that the disease could affect anyone.
“This outbreak highlights the urgent need for leaders to strengthen pandemic prevention, including building stronger community-led capacity and human rights infrastructure to support effective and non-stigmatizing responses to outbreaks”, he noted.
The agency urged all media covering Monkeypox to follow WHO’s updates.
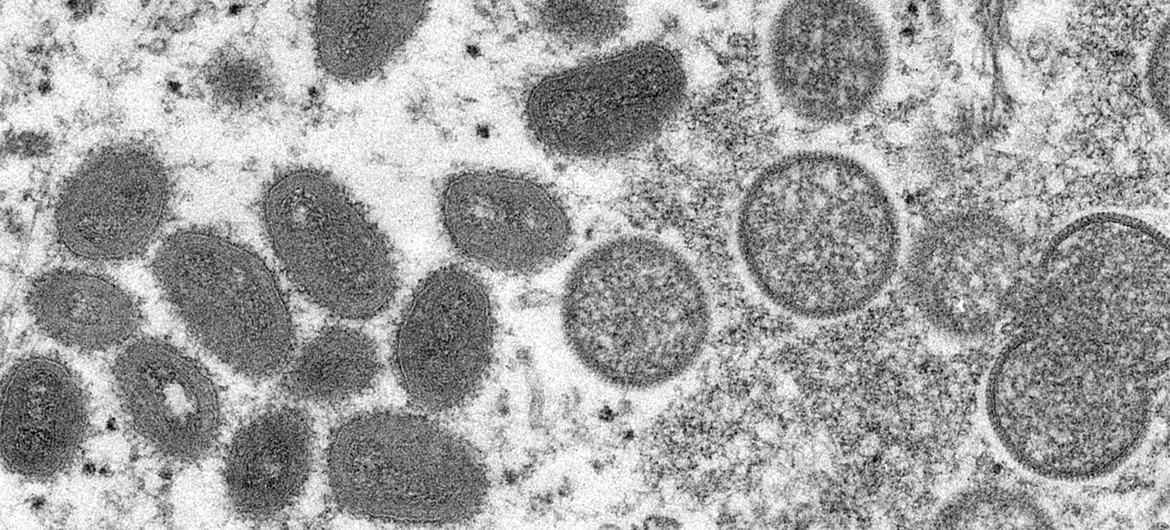
Monkeypox is a rare but dangerous infection similar to the now eradicated smallpox virus.
More cases expected
The UN health agency said over the weekend that as the situation is evolving and the surveillance expanding, it is expected that more Monkeypox cases will be identified.
To date, all cases whose samples were confirmed by PCR have been identified as being infected with the West African clade.
Genome sequence from a swab sample from a confirmed case in Portugal indicated a close match of the Monkeypox virus causing the current outbreak, to exported cases from Nigeria to the United Kingdom, Israel and Singapore in 2018 and 2019.
WHO said that the identification of confirmed and suspected cases of Monkeypox with no direct travel links to an endemic area represents a ‘highly unusual event’.
CDC
A young man shows his hands during an outbreak of monkeypox in the Democratic Republic of the Congo. (file)
About the illness
Monkeypox is a viral zoonosis (a virus transmitted to humans from animals) with symptoms very similar to those seen in the past in smallpox patients, although it is clinically less severe.
There are two clades of Monkeypox virus: the West African clade and the Congo Basin (Central African) clade.
The name Monkeypox originates from the initial discovery of the virus in monkeys in a Danish laboratory in 1958. The first human case was identified in a child in the Democratic Republic of the Congo in 1970.
Monkeypox virus is transmitted from one person to another by close contact with lesions, body fluids, respiratory droplets and contaminated materials such as bedding. The incubation period of Monkeypox is usually from 6 to 13 days but can range from 5 to 21 days.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.





















")